Situation Overview
A novel coronavirus appeared in Wuhan, China, in December 2019 and became more widespread by the middle of January 2020. The virus is a novel, or new, form of the relatively common coronavirus and has symptoms similar to that of SARS. The World Health Organization (WHO) named the virus SARS-CoV-2 because of the similarity in symptoms to SARS and the pneumonia it causes COVID-19. By late January, the Chinese government began aggressive quarantine measures impacting millions of people in an attempt to contain the virus. The WHO declared a Public Health Emergency of International Concern on January 30 followed by the US declaration of a National Public Health Emergency on January 31st. By the end of January, the total number of cases worldwide stood at 11,950 with 259 deaths.
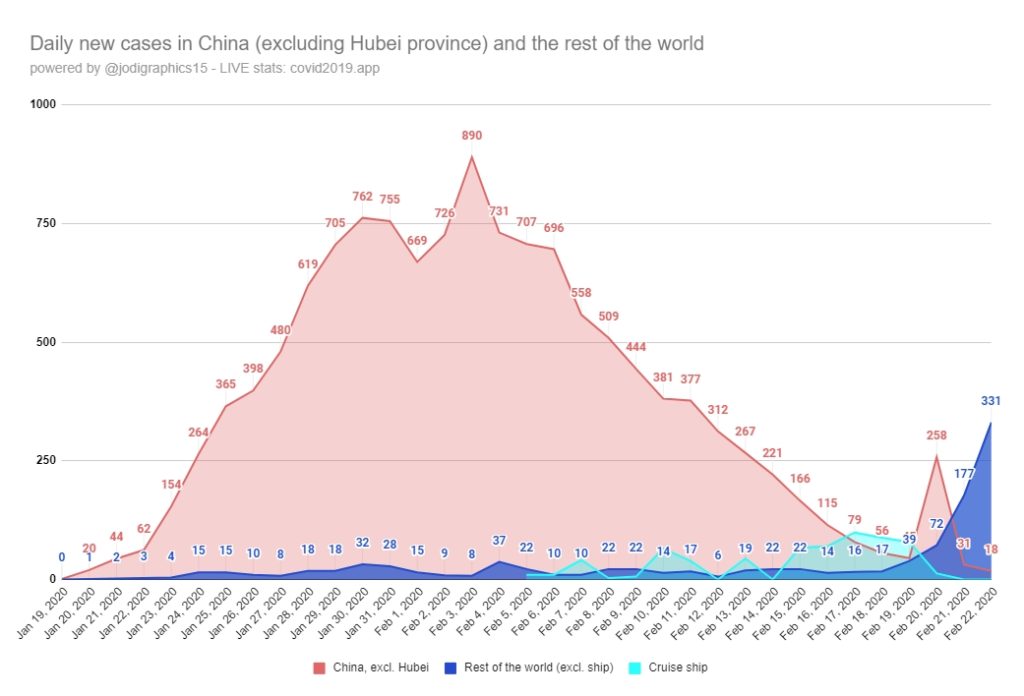
On February 19th, 2020, cases outside of the China jumped significantly with South Korea and Italy reporting the biggest spike in new cases. Additionally, it is suspected that a significant outbreak was occurring in Iran and North Korea although those countries are not reporting or underreporting cases for political reasons. This spike in new cases outside of China indicates that the novel coronavirus has become a global pandemic, spreading in multiple countries in multiple continents. As of the writing of this alert, the WHO has yet to declare the virus a pandemic, but is likely to do so in the coming days. Both the WHO and the US Centers for Disease Control (CDC) have been slow to take bold actions against in the coronavirus in an effort to minimize panic and maintain the global economy. However, more dramatic actions will soon be needed across the globe.
As of the writing of this alert on February 23, 2020, global cases of coronavirus stands at 78,987 infected and 2,470 deaths.
Virus Overview
The coronavirus is a family of viruses that causes a variety of illnesses ranging from the “common cold” in humans to respiratory infections in chickens and diarrhea in pigs or cows. This novel or “new” coronavirus is a brand new virus and is not SARS, although its namesake was given because the symptoms it causes are similar and it’s cause by the same family of virus. Because this is a new virus, the human body does not have any natural immunity to it and therefore, the infection can be more severe than viruses such as seasonal influenza or other coronaviruses that the human body is familiar with.
The novel SARS-CoV-2 coronavirus spreads via a variety of mechanisms, including:
- Airborne – Chinese officials have stated and anecdotal evidence from the Diamond Princess cruise ship suggest that SARS-CoV-2 can spread via nuclei in the air. This means that you can be infected from an individual more than 6 feet away and even via ventilation systems in buildings from infected patients in other rooms.
- Direct Contact – The virus can certainly be transmitted via direct contact, such as hand shaking, kissing, etc. with infected individuals. The virus can also be transmitted by saliva droplets in the air that are emitted by the infected via coughing, sneezing or talking.
- Surface Contact – The virus can certainly be transmitted via indirect contact with surfaces that have been contaminated by touch or droplets from coughing, sneezing or talking by infected individuals. The virus can survive on these surfaces for a day to several days depending on temperature, sunlight, and a variety of other factors.
- Feces & Urine – Preliminary studies (as well as evidence from SARS) suggest the virus can be spread through feces and urine as well as the aerosolization of these substances through flushing or urinating into a urinal or toilet.
The basic reproductive number (R0) for the novel virus is not yet known due to inexact reporting by China and other countries . The R0 is the number of people the average infected individual is likely to infect. Most studies suggest an R0 of 2 to 3 with some studies suggesting an R0 of near 4. By comparison, the seasonal flu has a an R0 of ~1.3 and the R0 of the 1918 Spanish Flu Pandemic that killed more people than WWI had an R0 of 2.
The case fatality rate (CFR) of the novel virus is also unclear due to inexact reporting, but is approximately 3% based on current “official” numbers. By comparison, the seasonal flu has a CFR of less than 0.1% and the CFR of the 1918 Spanish Flue Pandemic had a similar CFR of between 2-5%.
Therefore, the novel SARS-CoV-2 coronavirus is perhaps more contagious than the 1918 Spanish Flu, but perhaps slightly less fatal.
Some additional considerations with novel SARS-CoV-2 coronavirus is that the incubation period is long, generally between 7-14 days, but as much as 28 days, with some studies suggesting that the most infectious periods several days PRIOR to symptoms. Additionally, the fact that many people infected with novel SARS-CoV-2 coronavirus have only mild symptoms increases the potential for “super-spreaders” that can infect many more than the 2-3 people suggested by the average R0.
Community Preparedness
Regardless of the case fatality rate (CFR), official numbers suggest approximately 20% of cases will be severe and require oxygen therapy and ioslation. This number far exceeds the capability of most communities to provide medical care for an outbreak of COVID-19. For example, if there are 10,000 cases in metropolitan area that means 2,000 patients would require oxygen. This would overwhelm most local healthcare systems as they are only prepared to handle slightly more than normal patient loads and only maintain a limited supply of personal protective equipment.
Finally, a large number of people not reporting to work out of fear, quarantine, and mild cases in isolation will likely cripple many critical systems. This includes the delivery of groceries, medications, and other goods, maintenance of utilities and communications systems, and the delivery of critical services including police, fire/rescue, healthcare, garbage collection, etc.

